{Life-Changing Plastic Surgery Stories} “I Looked Like A Melting Snowman!”

![]()

Karen B., 62, vividly remembers report card day in sixth grade. “In those days, your grades were listed with your height and weight,” Karen explains, and the teacher would read them out loud as he handed the report to you. “I remember jumping out of my seat and running to his desk in tears, begging him not to read mine.” Karen was 12 years old and 126 pounds. “I was the biggest girl in the class. Always,” she says.
Smart and ambitious, Karen excelled in school, eventually earning a B.S. in chemistry and becoming a nurse. She married a Marine in her early 20s and they had two children while he built a successful business. Through it all, Karen felt powerless over her weight, which fluctuated between 220 and 280. “I would diet, work out and then gain it back,” she says. Finally, in 1989, she had gastric bypass—then a new procedure—and lost 120 pounds. “But the brain is funny thing,” she relates now, “and you can find ways to circumvent the surgery and eat what you want.” Over the next two decades, the weight crept back. “When I retired three years ago, I was hanging out at about 215.”
Then, during a routine physical, Karen was diagnosed with diabetes. Shocked and upset, she spent the next year researching on the internet. “I found a good diet and a trainer at LA Fitness. I also started taking Byetta, a diabetes medication.” Over the year, the weight came off steadily. “I hated working out. Hated it,” Karen laughs. But ultimately, her weight got down “to the low 140s” and stayed there for two years.
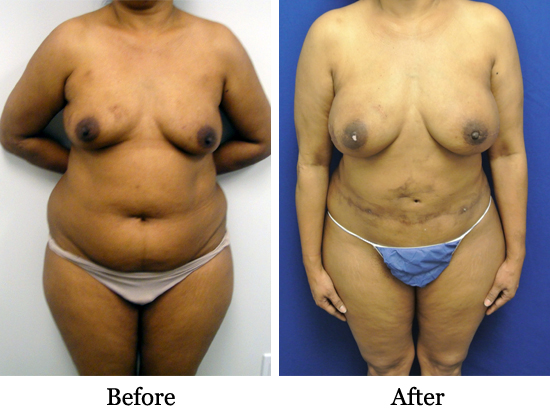
Now at her “perfect weight,” Karen was thrilled, but when she looked in the mirror, she saw “all these sags. I looked like a melting snowman. My 10-year-old granddaughter would say, ‘I love your arms, Grandma!’ and would swing the skin back and forth!
“I didn’t want to grow up to be a saggy, saggy old lady,” Karen says. So she asked a friend who was in a gastric bypass support group if anyone had come to talk to them about plastic surgery. “She gave me Dr. Boynton’s name and said he seemed wonderful. So I called his office.”
Ten months and two surgeries later, and the results speak for themselves. “I want to run through the mall naked!” Karen laughs. “I have not stopped smiling.” Here, she explains the details of what Dr. Boynton did to give her “a body I never in my wildest dreams thought I would have.”
Tell me about your first meeting with Dr. Boynton.
First of all, the thought of showing someone an old body with all this saggy droopy skin on it made me want to die of embarrassment! I’ve spent my whole life trying to tuck it in and not show it. But you walk in his office, and everyone is so nice. He meets with you while you’re dressed, so you can get to know him. He tells you about his philosophy and his training, and you can just feel that he has a good spirit. I thought, ‘I can handle this!’
What surgeries did you have?
Dr. Boynton likes to do things in stages. He’s very careful, which I like. The first surgery was a tummy tuck and some liposuction on my flanks and lower back. He told me he likes to start with the tummy—the core. After having two babies my muscles were spread apart, so the muscle repair was a big deal. He did a breast lift in round two, as well as a breast augmentation and my upper arms.
How was the recovery?
Surprisingly easy. Dr. Boynton had explained that he was using Experil, a new drug that keeps you comfortable for 72 to 96 hours after the surgery. He injects the drug along the muscles and the incisions during surgery so when you wake up you really feel great. I’m a geek, so when he told me about it I went on YouTube and watched procedures being done. I was very impressed. After the first recovery, I asked him if he could use Experil again when he did my breast augmentation and he actually researched it and learned the technique for breasts at my request. I couldn’t believe he did that.
When were you able to get up and leave the house?
One and a half weeks after the second surgery I went to the mall, still with my compression garment on, because I wanted the woman at Victoria’s Secret to measure me. I wanted to see what size I was. She couldn’t believe I was out. She said, ‘no one is up like this two weeks later!’
So what is your new size?
Well, I went to Black House White Market the other day and I bought a new pair of pants, because literally everything is falling off of me. And they were a size four. A four! I’m someone who used to be over the moon about a size 10. I showed my husband and he was like, ‘did you ever in your wildest dreams think you’d be a size 4?’
What’s your husband’s reaction to all of this?
My husband is the most wonderful person. He has told me my whole life, ‘I love you no matter what you weigh.’ And he has loved me unconditionally no matter what. What makes him happy now is seeing how happy I am. That’s the kind of guy of guy he is. I said ‘honey, you have your trophy wife and you didn’t even have to get divorced and lose half your money to get it.’
What about friends? What do they say?
People who haven’t seen me for a while have said, ‘Oh my god, what have you done?’ And I just say, ‘I lost some weight and I kept it off and I had a little something something done.’ And then I hand them Dr. Boynton’s card. I went back to see my co-workers after my tummy tuck and they could not believe it. Three of them asked for his card.
Do you plan to have any more surgeries, or are you done?
In the fall we’re going to do legs and butt—get the sags off and finally finish it. We’re not quite there, yet, but as long as Spanks exist I can fake it til I make it!
What’s your overall impression of Dr. Boynton?
I have worked with hundreds of doctors over my 32 years as a nurse and assisted on many surgeries, and I can tell you he is number one in every respect. I feel like I am in such competent hands. But more than that, he’s very real and down to earth. You can talk to him. One day I came into his office with my 10-year-old granddaughter. She has a lot of physical disabilities, and the first thing he said when he saw her was, ‘You have pink river shoes on!’ And that just melted my heart, because most doctors—especially surgeons—won’t do that. They are too rushed and harried and they have no bedside manner. His heart is right there.
And trust me, you never want to go to a doctor that a nurse wouldn’t go to!
What would you tell an FOF who was considering surgery?
It’s never too late. I’m an evangelical Christian, and I remember going to a big camp meeting in 1981 with a popular evangelist minister. He had everyone close their eyes and think about the desire of their hearts. Mine had always been to be a normal size. He said, ‘I will pray for everyone here, and if you hang onto that, it will happen.’
Well, it took 32 years—diabetes, exercise, bypass surgery. It wasn’t overnight, but all this time has made me appreciate it that much more. I mean, unless you’ve lived in double your body, I don’t know if you can really appreciate size-four pants. This is the first time ever in my life that I actually feel desirable and alive and sexy. Before, that wasn’t even in my realm of awareness.
![]()