
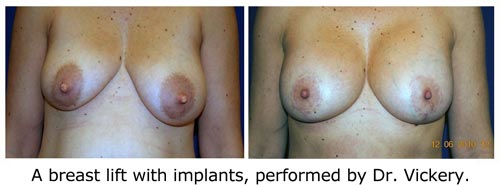
Great breasts after fifty
If you think beautiful breasts are a thing of the past, Dr. Carlin Vickery says, think again.
When we hear “breast surgery,” most of us think of Hollywood starlets, porn stars or Pamela Anderson. But statistics show that FOFs–regular women with jobs, brains and no big-screen ambitions–are having more cosmetic breast surgeries than ever before.
Why the sudden trend? “We’re entering an era where women are going to be living a long time,” says Dr. Carlin Vickery, a board-certified plastic surgeon and one of Manhattan’s most sought after sources for breast lifts and reductions. “The quality of our lives is going to be dictated by our physicality. Being able to stay active and fit will actually extend and improve our lives.” And for many women, that means lifting and/or reducing their post-menopausal bazooms.
We spoke to Dr. Vickery about breast surgery and why FOFs are such good candidates.
- What happens to our breasts as we age?
- As we go through childbearing, nursing and menopause, most women will lose skin elasticity. So there is a natural gravitational descent of the breast gland, which can result in droopy breasts, or, as we call them, ptotic breasts. In addition, with a loss of estrogen, the breast tissue will become more fatty, which leads to a loss of volume, especially at the top of the breast, which, in our culture, is the desirable cleavage area.
- Do breasts generally get larger, or smaller over time?
- It depends on the woman. Some women, after having children, experience post-partum involution, meaning the breast tissue just shrinks down. That’s very common; I see it in a number of women in their 40s and 50s. Other women’s breasts get larger.
- What are the most common types of breast surgery for women over fifty?
- Women usually come in complaining of sagginess and a loss of volume. They need breast lifts–and that can be done with or without an implant, depending on whether the patient needs more volume. Breast reductions are the other popular precedure for the over-fifty group.
- Do you think most FOFs come in with realistic expectations?
- I think they do. A lot of younger patients come in wanting something they’ve seen on TV or wanting tons of cleavage. But women over fifty are more mature and realistic. They have a good idea of who they are and many have waited a long time for this. Often, they feel like their breasts are too big and are making them look matronly–fat and top heavy. If anything, they want their breasts to be too small.
- Is there such a thing as “too small” breasts?
- I’m a big believer in proportionality. You never want to reduce breasts so much that your belly is leading your profile. That’s not a desirable look, and it’s going to makes clothes harder to fit.
- Let’s start with the breast lift. Does it always require an implant?
- No–not necessarily. You can lift the breast, but without an implant, you’re not going to get that volume that most women are looking for.

- No–not necessarily. You can lift the breast, but without an implant, you’re not going to get that volume that most women are looking for.
- Do you have a preference for silicone versus saline implants?
- I don’t. That’s a decision the patient needs to make, and my job is to give them all the advantages and disadvantages of both. I will say that the gel implant often has a slightly softer feel–but not always. For a while, silicone was under suspicion of causing autoimmune disease, so we all used saline implants, and people were very satisfied.
- What’s the biggest misconception about breast implants?
- People don’t realize that implants require maintenance over time. The FDA has now deemed silicone implants safe, however they need to be replaced every 10 to 15 years.
- What’s the most popular procedure right now for achieving a “natural” look with an implant?
- There’s not one. To be a good plastic surgeon, you have to be flexible, and you have to have a big bag of tricks. If you’re doing the same procedure on every patient, then you’re not achieving the best results. Two women complaining of “sagging” could have completely different anatomy: is the problem lost elasticity, or are the nipples pointing down, or do they have stretch marks, or do they have great skin with a loss of volume? If a doctor says he has one technique that he always, uses, then . . . I can’t get my mind around that.
- If you look on the internet, you will find doctors who are practicing these large-volume fat injections. I think the jury is still out on this procedure. I have seen some good results in photos, but there’s a lot of variation. And there’s concern about whether injecting fat into the breast can prevent effective cancer screening, or if there are biological risks to that injected fat. I think fat injection is the future–we’re just not quite there yet.
- The most important thing: Is the doctor listening to what you’re saying? A good plastic surgeon really listens to the patient and attempts to understand the patient’s goal and whether or not they have a surgical technique that’s going to reach that goal.
- There are a lot of things–some of which you can control and some you can’t! Large-volume weight gain and weight loss stretches out the skin you’re apt to get sagging. Wear a good, supportive bra that minimizes repetitive jiggling, especially when you’re jogging and exercising. Smoking is going to hurt the elasticity of your skin–not just your face, but also on your chest wall. Spending a lot of time in the sun will also decrease elasticity and cause breasts to sag.
- I personally don’t know any that work. It’s not the answer people want to hear, but the fact is, anything that helps you stay more fit overall–exercise, diet–will help preserve your breasts as well.
- A few reasons. After menopause, we tend to put on weight in our mid-section, so many women complain that they feel top-heavy. Also, if you have large breasts, it’s a major drag on your upper skeleton–particularly your neck shoulders and back. As women age, they can develop deep grooves their bra straps are, back pain, headaches, etc. If you’re prone to osteoporosis, it puts strain on your back and can exacerbate the problem.

- Absolutely. Women who have the procedure tend to immediately feel better and lighter. Still, there are women who feel almost like they have to apologize for coming in and asking for a breast reduction. Why?! You don’t have to apologize–this makes perfect sense. You’re 55 years old, and these breasts are pulling on you 24/7 and you want to be able to go to the gym do yoga.
- I think most women are shocked by how much younger and thinner they look after the surgery. Most of my patients who have this procedure say, “I can’t belive I waited so long!” I think people are also surprised by how well tolerated this procedure is. A breast reduction typically requires a few days of recovery and some Percocet! In plastic surgery, we often say breast reduction patients are our happiest patients.
- There is a group of patients for whom I belive their longevity and the quality of their lives would improve if they had breast reduction. Sometimes I have to sit on my hands, because I see women who would really benefit from it. But I’ve never figured out how to have the conversation with someone who’s not a patient. I just think, ‘I could really help that woman!’
| Author | |
 |
Plastic surgeonDr. Carlin Vickery, MD, F.A.C.S., has been practicing surgery for over 25 years. Consistently ranked as one of New York City’s top plastic surgeons by Castle Connolly Medical, Dr. Vickery has pioneered innovative approaches to breast reconstruction and augmentation. She holds an appointment as Associate Clinical Professor in Department of Surgery at Mount Sinai Medical Center, where she has taught since 1985. |
 e don’t realize that the FDA hasn’t issued any new sunscreen safety regulations for more than 30 years,” says Nneka Leiba, a research analyst who worked on
e don’t realize that the FDA hasn’t issued any new sunscreen safety regulations for more than 30 years,” says Nneka Leiba, a research analyst who worked on 

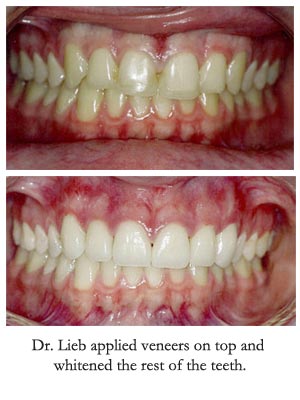 Do you see a lot of shifting teeth in women over 50?
Do you see a lot of shifting teeth in women over 50?
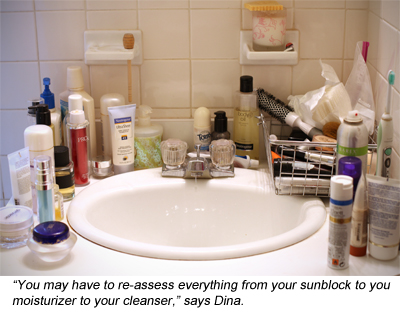 You want to protect and soothe your skin. Use a very gentle, non–foaming, milky cleanser. La Roche Posay makes an over-the-counter cleanser called Lipikar that I like a lot. A lot of doctors recommend Cetaphil but it has propylene glycol which I’ve noticed can be irritating to my sensitive FOF patients. Choose a moisturizer with antioxidants to protect the skin during the day. I like Active C, also OTC from La Roche POsay.
You want to protect and soothe your skin. Use a very gentle, non–foaming, milky cleanser. La Roche Posay makes an over-the-counter cleanser called Lipikar that I like a lot. A lot of doctors recommend Cetaphil but it has propylene glycol which I’ve noticed can be irritating to my sensitive FOF patients. Choose a moisturizer with antioxidants to protect the skin during the day. I like Active C, also OTC from La Roche POsay. What the biggest mistake you see women making after fifty?
What the biggest mistake you see women making after fifty?



