7 Things We Must Have In Our Handbags at All Times
1. Burt’s Bees
“Burt’s Bees Pomegranate Lip Balm” —Jeanie Scoggins Williams“Burt’s Bees lip shimmer” —Diane DiBiase“Burt’s Bees.” —Barbara Fritz


1. Burt’s Bees
“Burt’s Bees Pomegranate Lip Balm” —Jeanie Scoggins Williams“Burt’s Bees lip shimmer” —Diane DiBiase“Burt’s Bees.” —Barbara Fritz


We know you’re out of school, but we have a fun assignment for you. Using the examples from Geri, Melissa, La Toya and Annette–send us side-by-side photos of you, from “then” and “now.”
Tell us what’s changed and what hasn’t. Or just send photos and captions. Whatever suits your FOFancy!
We want to know about YOU.
We’ll post Then & Nows on our site! Stop reading and get to work! Completed assignments can be sent to alex@faboverfifty.com.
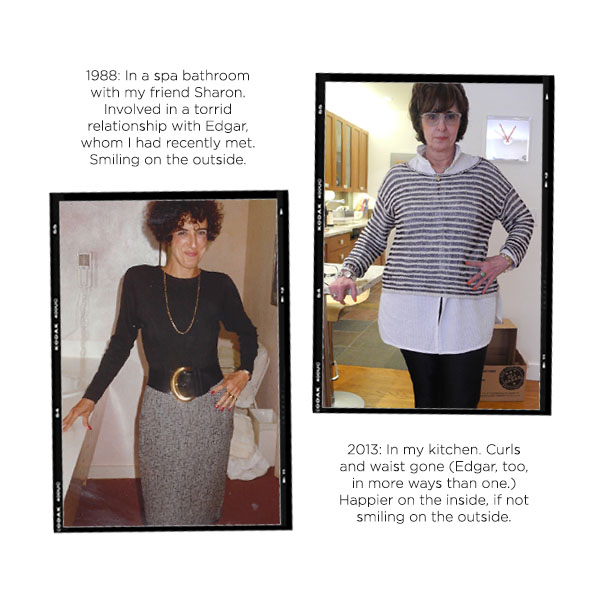
Then @ 41
“I had recently lost 50 pounds—went from 177 to 127—and just loved my svelte new body. So everything I bought was form fitting. Notice the slim skirt and spandex like top. I also wore heels, even though my feet were killing me. Needed to show off those legs. The wide belt was a Donna Karan from Barney’s (before it moved uptown and became ridiculously pretentious.) I still have the belt, in red, too. It now fits around half my waist. I remember everything about the belts because I bought them when my father was dying.”
Now @ 66
“I won’t tell you what I weigh, but suffice it to say, it’s more than 127. So I now cover my bigger tummy and thighs with ample tops. I love leggings because they’re slimming and cover the cellulite, too. I never wear heels. I think flats are sexy, and I don’t risk toppling over and killing myself, which is something to consider at FOF. My curls are gone and so is my thick hair, which I now cover with a marvelous piece from LeMetric, which is owned by my dear friend, Elline. I’m forever trying to lose 20 pounds but I refuse to stop eating certain foods I enjoy. Nevertheless, I like my style—and myself—more than I ever have.”
Send your Then & Now photos and comments to alex@faboverfifty.com!

—————————————————————————————————
 FOF Connie Sherman is giving away a “cooling” Hot Girls Pearl Necklace and travel purse. Enter to win by answering in the comments below: Do you own a set of pearls?
FOF Connie Sherman is giving away a “cooling” Hot Girls Pearl Necklace and travel purse. Enter to win by answering in the comments below: Do you own a set of pearls?
When FOF Connie Sherman turned 47, her doctor found “questionable cells” in her breast tissue and put her on Tamoxifen. The medication came with an unpleasant side effect–frequent, agonizing hot flashes. “I’d literally come home and stick my head in the freezer,” says FOF Connie Sherman, now in her sixties.
Two years ago, still heated about her hot flashes–Connie began to think about out-of-the-box solutions. A former creative director in NYC for Harper’s Bazaar, Vogue and Bloomingales, fashion was always on Connie’s mind. “I wanted something I could wear, that would actually do something about the heat,” says Connie. “And I’m not talking about a bandana.” She got to work on a prototype for Hot Girls Pearls, jewelry made from beads filled with the same non-toxic icy gel that’s in medical ice packs.
Last June, when she was satisfied with her prototype, Connie rolled out her Hot Girls Pearls necklace in three sizes (16”, 18” and 19.5”) and a bracelet. More recently, she has added two new colors to her line: gunmetal and dusty pink. Her pearls start at $30.
Connie’s cool jewelry has proven a hot commodity–they’ve been featured on ABC’s The View, The Today Show and in Oprah’s O Magazine. Connie estimates she’s sold 5,000 Hot Girls Pearls in less than a year. “There’s not one woman who doesn’t sigh in relief when they put them on,” says Connie.
Enter to win a Hot Girls Pearl Necklace and travel purse invented by FOF Connie Sherman by answering in the comments below: Do you own a set of pearls?
—————————————————————————————————
One FOF will win. See all our past winners, here.) (See official rules, here.) Contest closes May 3, 2012 at midnight E.S.T.
Thank you for entering. This contest is now closed.

A screenshot from “Anyone can wear a white coat,” an alarming PSA about plastic surgery, courtesy of the ASPS. Click here to see the complete video.
—————————————————————————————————
.
“In many ways, plastic surgery is still the Wild West in this country. Any physician can legally call him or herself a plastic surgeon. Your family doctor can decide, ‘I think I’ll do facelifts today.’ It’s vital to do your homework to get the best doctor, best procedure and best outcome.”
–Dr. Malcolm Roth,plastic surgeon and President of the American Society of Plastic Surgeons
Everyday we get questions from FOFs about plastic and cosmetic surgery. Everything from, “What is the least invasive face lift procedure?” to “Is it safe to have plastic surgery in Mexico?”
This year, we’re partnering with the American Society of Plastic Surgeons (ASPS), a not-for-profit authority on plastic surgery and plastic surgeons–and an organization we trust–to bring you the very best information on this topic.
This week, we interviewed Dr. Malcolm Roth, Chief of Plastic Surgery at Albany Medical Center, and the president of ASPS, who explains exactly how to find the right doctor, and why it can be confusing. “It’s vital for every FOF to do her homework before she chooses a doctor or a procedure,” says Dr. Roth. Our advice: If you’re considering any cosmetic procedure (including injections, lasers or even hair removal) read this first.
FOF: Why is it so confusing when it comes to choosing a qualified plastic or cosmetic surgeon?
Dr. Roth: In this country, any physician can legally call himself a plastic surgeon, even though he may not be board certified in plastic surgery. In most states, he can even advertise that he’s board certified and a cosmetic or plastic surgeon (though he may not be board certified in plastic surgery). So your gynecologist or family doctor can decide, “I think I’ll do facelifts today,” or “I think I’ll do liposuction.” As long as you have an office where you can perform the procedure, you can do what you want to do. There are some exceptions to this rule in a handful of states, but generally speaking, all you need is a facility and a medical license to perform surgery.
Wow. Why would a doctor who is not trained in plastic surgery decide to do it?
It’s difficult surviving in the world today as a physician. Insurance companies are decreasing their payments for procedures and making it more difficult to get paid. It’s easier to say, ‘Why not just do plastic surgery? My patients will pay me cash up front, and it looks easy.’ A cosmetic procedure can sound simple, but, even something like liposuction, in the wrong hands, is very dangerous. We’re hearing more and more about serious problems, and all ASPS members are seeing unhappy patients who need reconstruction, or are even beyond the point of reconstruction, due to surgery performed by unqualified physicians.
What is ASPS and how are its doctors qualified?
We are the largest plastic surgery specialty organization in the world. Our 7,000 cosmetic and reconstructive plastic surgeons are board certified by the American Board of Plastic Surgery. That means they have completed 6 years of surgical training with at least three of those years specifically devoted to plastic surgery. To qualify for ASPS, you must operate only in accredited medical facilities, adhere to a strict code of ethics and fulfill continuing medical education requirements to stay up to date, especially on patient safety. We are a non-profit, and our mission is to advance quality and, most importantly, safety, in plastic surgery.

Why is this important to FOFs?
You know the old expression, if the only tool you have is a hammer, everything looks like a nail? Our surgeons have all the tools in the tool chest. If you’re a family doctor who has taken a weekend course in injectables, you’re going to recommend injectables to your patients, even if there are better options. Our members understand all the options, appropriate facial aesthetics, and most importantly, safety. They know what to do when something goes wrong.
For our society and our members, this isn’t a turf war. This is about trying to make sure patients understand that they have a choice and a responsibility to do their homework.
Okay, so how does an FOF do her “homework?” How do you choose a doctor who is skilled, safe and has the maximum amount of training?
Here are the key questions every woman should ask a plastic surgeon she is considering:
.
.
.
.
.
.
.
.
For facelifts, lipo and other surgical procedures, it makes sense to use a plastic surgeon. But what about injectables? Is it okay to go to a dermatologist for that?
Fillers and neurotoxins and other minimally invasive procedures are within the scope of dermatologist training, and it’s certainly reasonable to go to a dermatologist for those things. However, remember that dermatologists are not trained to do the surgical procedures that our members are trained to do. So if your dermatologist offers you filler, that’s probably fine. If, on the other hand, they suggest, “Well, how about I do a facelift?” that’s not in the scope of their training and a better option would be for you to consider an ASPS member surgeon.
Also, a plastic surgeon is going to know every nook and cranny of the face–where the nerves are, and what the ramifications are if you injure a nerve you’re not supposed to. An ASPS member will know how to minimize the risk of injury to vital structures. Injectables aren’t just a “skin procedure,” and it’s valuable to have somebody who has full understanding of the underlying anatomy.
What is the ultimate “red flag” that should send you running from a doctor’s office?
If they’re not trained in plastic surgery, you’ve got to be crazy. Run away. And if they are trained, but you don’t feel like you and the surgeon are connecting…that’s not a good sign. Find someone else. There’s no rush–this is your life you’re talking about.
Visit plasticsurgery.org to start your search for a qualified plastic surgeon in your area.
Is this the one vice every FOF needs to give up . . . now?

—————————————————————————————————
 When Dr. Vincent Pedre, MD, one of New York City’s most sought after internists, meets a new patient, he always asks her: “How much soda do you drink? How much diet soda do you drink?”
When Dr. Vincent Pedre, MD, one of New York City’s most sought after internists, meets a new patient, he always asks her: “How much soda do you drink? How much diet soda do you drink?”
“I don’t wait for her to volunteer the information,” says Pedre. “Soda consumption is an important part of the overall health history.” The fact is, millions of us drink diet soda because we’re (a) trying to lose weight; (b) like it more than water; and (c) compared to soda, it’s the lesser of two evils . . .right? Wrong, says Dr. Pedre, who insists that diet soda is just as bad if not worse for your body…and for your waistline. Here, he offers seven reasons to stop drinking it right now.
1. It actually makes you fatter.
Scientists at the University of Texas Health Science Center San Antonio followed 474 people for 10 years and found that the more diet soda the subjects drank, the fatter they got. Diet soft drink users experienced 70 percent greater increases in waist circumference compared with non-users. Those who drank two or more diet sodas a day saw their waists grow 500% bigger than non-users, even when controlling for things like age and exercise. Wait . . . what? How could America’s favorite diet drink be making us fat? “We still don’t know for sure, why,” says Dr. Pedre. “One theory is that when you eat something sweet, it triggers insulin and the cascade of hormones that make you feel full. Diet soda triggers the sweet receptors on your tongue, but not the insulin, so you never feel full. It actually causes you to crave–and probably eat–more high-carb, processed foods.”
2. It increases risk of stroke, heart attack and cardiovascular disease.
A recent study of 2,564 adults over 40 living in Manhattan (published in the Journal of General Internal Medicine) concluded that daily consumption of diet soda was independently associated with an increased risk for stroke, heart attack and death. Shockingly, consumption of regular soda was not associated with an increased risk. “Again, this doesn’t tell us why,” says Dr. Pedre, “but we know that people who drink diet soda seem to gain weight and have a greater chance of developing metabolic syndrome,” an increasingly common syndrome associated with abdominal weight gain, high blood pressure, high blood sugar, insulin resistance, an increased risk for heart disease and diabetes.
3. It gives you a super-powered sweet tooth.
“The level of sweetness in these diet drinks–the strength with which they stimulate your sweet receptors–is so strong, that you can lose the ability to taste the natural sweetness in foods like fruits and vegetables,” says Dr. Pedre. “You end up wanting to eat things that are going to stimulate those receptors, such as processed foods and other sweets. When you put someone on a detox, and take these things out of their diet for a while, their taste receptors come back. Suddenly they’re able to eat a blueberry, which maybe tasted bland before, and appreciate how delicious it is.”
4. It leaches calcium from your bones.
Diets high in phosphoric acid are associated with lower bone density, hip fractures and osteoporosis. Guess what contains phosphorous? That’s right, cola. Phosphoric acid gives your diet Coke that tangy, acidic taste that’s so fun to drink, plus it prevents mold and bacteria from forming in the can. Yum? “The addition of caffeine also causes reduced calcium absorption,” points out Dr. Pedre. “If you’re drinking a diet cola or two a day, you’re really setting yourself up for osteoporosis in the long run.”
5. Some experts insist that artificial sweetener is a neurotoxin.
The debate has long raged as to whether artificial sweeteners cause cancer. “It’s fine!” says your friend as she swirls five Equals into her coffee. “That answer is still up in the air,” admits Dr. Pedre, “But, aspartame is a neurotoxin, which means it causes irritation and over-stimulation of the nerves.” This is also a highly controversial statement. The FDA has assured consumers that aspartame is safe, however the debate has raged on, and in recent years many European brands have been slowly removing aspartame from their products. In addition, a minority of very vocal doctors, including Dr. Joseph Mercola, a Huffington Post blogger, and Dr. Russell Blaylock, a board certified neurosurgeon, have led crusades against the additive, insisting that it causes longterm nerve and neurological damage, with common symptoms being headaches and migraines. According to a widely quoted article by Dr. Mercola, “100 percent of the industry funded studies supported aspartame’s safety, while 92 percent of the independently funded studies identified at least one potential health concern.”
6. The caramel color is a carcinogen.
Coca Cola and Pepsi both use a chemical called 4-methylimidazole (4-MI) to give their drinks that signature brown, caramel color. Looks yummy, but 4MI is a known carcinogen that, in high doses, has been linked to cancer in mice and rats. As part of California’s new Proposition 65, a company must inform consumers if its products contain any substance “known to cause cancer or reproductive toxicity.” Reluctant to put a “toxic” warning on millions of cans, Coca Cola released a statement this week saying: “We have asked our caramel manufacturers to modify their production process to reduce the amount of 4-MI in the caramel.” Is the additive gone? No. Is this language sort of hazy? Yes. “The FDA has let this slide because they say the quantity of 4MI in the sodas isn’t enough to be harmful,” explains Dr. Pedre, “But these toxins are stored in fat, so if you’re overweight or carry weight in your mid-section, I can tell you that you’re likely not flushing this toxin out of your body. Each time you drink a soda, more toxins are going in than are coming out. That cumulative effect is very hard to account for.”
Ready to crack open an ice cold cola? Yeah . . . we aren’t either. So what should we drink? “Water,” says Dr. Pedre. “I can also get on board with sparkling water and a touch of organic berry juice or lemon. Bottom line: If you drink water, herbal tea and eat lots of plants, you just don’t have to worry about this stuff.” How . . . refreshing.
Editor’s note: We’re curious . . . do you drink diet soda?
The FDA is adding new warnings to this popular drug. Here’s what you need to know now.

—————————————————————————————————
If you’re over fifty in America, there’s a good chance you’re taking a statin. Nearly 22 percent of adults 45 or older take one of these cholesterol-lowering drugs, making them the most commonly prescribed medications in the world.
Last week, the FDA added new safety alerts to statin labels, including reported side effects of memory loss, confusion, and a higher risk for Type 2 diabetes. Not surprisingly, many people panicked. Medical message boards were flooded with questions like, “Will Zocor give me dementia?” and “Is Lipitor making me sick?” A cursory google search brings up dozens of sites claiming statins are dangerous, unnecessary, over-prescribed—even a corporate conspiracy. Still, the FDA insists that this new information should not “scare people off statins. The value of statins in preventing heart disease has been clearly established. Their benefit is indisputable.”
 So what’s the real story? For answers, we turned to a source we truly trust, Dr. Steve Nissen, Cleveland Clinic Chairman of Cardiovascular Medicine. Named one of Time magazine’s 100 most influential people, Dr. Nissen is not only a leading cardiologist and researcher, he’s also a leading patient advocate. He has has led inquiries as to the scientific integrity of many big-name medications currently on the market. In other words, he’s not afraid to question the status quo. Here, he answers all our questions.
So what’s the real story? For answers, we turned to a source we truly trust, Dr. Steve Nissen, Cleveland Clinic Chairman of Cardiovascular Medicine. Named one of Time magazine’s 100 most influential people, Dr. Nissen is not only a leading cardiologist and researcher, he’s also a leading patient advocate. He has has led inquiries as to the scientific integrity of many big-name medications currently on the market. In other words, he’s not afraid to question the status quo. Here, he answers all our questions.
FOF: If you are currently taking a statin medication, should you consider stopping as a result of this report?
Dr. Nissen: No patient should stop a medication because she hears a news report. These decisions should always be made through a discussion with your doctor. Most authorities do not believe that these new warnings represent a major change in thinking about statin drugs. We’ve known for several years, for example, that statins do very slightly push up blood sugar. That means, if you’re just under the threshold for diabetes, you’ll cross over and be labeled as having diabetes. But, in those patients for whom the blood sugar did go up a little bit, the benefits of the drug remained the same. The diseases that statins prevent–like heart attack stroke–are still reduced equally well.
Still, it’s alarming how many people are on statins. Do you think these pills are over prescribed?
I do. Doctors need to stick with the guidelines, which are very carefully worded so that patients at high cardiovascular risk are recommended for receiving statins, and patients who are at low risk are not. There are a certain number of people–I’ll call them the ‘worried well’–who are treated with statins by their doctors but who don’t really meet the current criteria. Those people are better off using diet, exercise and other means to control their cholesterol elevation. But, there are equally large numbers of patients who meet all the criteria for receiving a statin and who aren’t on them. The key is to make sure the right patients get these drugs.
How do you know if you should be taking a statin or if you’re one of the “worried well”?
There is a risk calculator available online called the Framinghan Risk Score. If you put in your numbers (age, cholesterol, blood pressure, etc) it will give you your 10-year risk of having a heart attack. If you come out well under 10% risk for 10 years, your risk is low, and you likely don’t need to be on a statin. If you’ve had a heart attack, you should be on a statin–period. If your LDL cholesterol reaches a certain level–above 160-190–we will treat you with a statin even if they have minimal other risk factors.
If your doctor says you need to be on a statin, but you are still concerned, what do you need to say to your doctor to make sure you’re getting the right treatment?
Ask exactly what calculations he or she using to determine your treatment. Did he or she use the Framingham or another similar tool? If you still have doubts, it is never a bad idea to get a second opinion.
What if you’re on a statin and you’re experiencing some of these side effects. Should you be worried?
Every drug has a degree of tolerability that differs from patient to patient. Good medicine is about customization. The goal is to find the drug in the dosage that works for you with the least side effects possible.
There are many sites on the web with experts who claim that these drugs are way over prescribed, and that there are “natural” alternatives to lower your bad cholesterol without jumping on a statin.
I have a very simple answer for those sites: nonsense. There are no “natural” alternatives to statins. The dietary supplement industry is unregulated, so they make these claims but there’s no science to back them up. Don’t be fooled by these promotions of dietary supplements—they simply don’t lower cholesterol.
So maybe there isn’t a supplement. But what about changing your diet and exercise? Can behavioral changes be a good alternative to statins?
A statin should always be coupled with behavioral changes. Good and prudent doctors always couple lifestyle changes with drug therapy. Using these behavioral changes as an alternative to a statin depends on your level of risk–every patient is a little bit different.
If you’re on the borderline of taking a statin, should these side effects be a motivation to make changes to your lifestyle so you don’t have to go one one?
It’s not that easy, and here’s why. Lifestyle changes typically don’t reduce cholesterol by more the 10-15 percent. Statins reduce cholesterol levels by 30-60 percent.If your numbers are high enough that you need a statin, the odds are good that you’re not going to get them down with diet alone, unless you’re willing to take on an extreme diet…and most people can’t sustain that.
Why would you be in a situation where your cholesterol levels are so high that there’s nothing you can do but take a statin?
It’s really about genes. Only 20 percent of cholesterol level comes from your environment…80% comes from your genes. That’s one reasons that diet can only lower cholesterol so much.
What about people who say that these drugs are being over-prescribed because of all the marketing being done by big pharmaceutical companies?
There’s a marketing element here absolutely. Having said that, we have probably saved more lives by lowering choesterol levels with statins than with any other drugs in the history of the medical profession. The only thing that comes close probably is penicillin.
If there is one single change you could be making to lower your bad cholestorol–apart from a statin–what would it be?
Reduce your intake of saturated fat in your diet–butter and meat.
A new report says yes, but another expert says . . .

—————————————————————————————————
“For decades, scientists have looked for explanations as to why certain conditions occur with age, among them memory loss, slower reaction time, insomnia and even depression. . . . Now, a fascinating body of research supports a largely unrecognized culprit: the aging of the eye.” —The New York Times, February 20, 2012
—————————————————————————————————
 FOFs are buzzing (and panicking) about last week’s article in The New York Times that examines a body of research from Dr. Martin Mainster and Dr. Patricia Turner, two ophthalmologists from the University of Kansas School of Medicine. Mainster and Turner claim that the gradual yellowing of the lens and narrowing of the pupil that occur with age prevent sunlight from getting through to key cells in the eye. They claim that this disturbs our circadian rhythms–the body’s natural clock–and leaves us at greater risk for a number of ailments, including insomnia, heart disease, cancer and depression. Their evidence is compelling: Based on their research, Mainster and Turner estimate that by age 45, the average adult receives just 50 percent of the light needed to fully stimulate the circadian system. By age 55, it dips to 37 percent and by age 75, to a mere 17 percent. “We believe the effect is huge,” says Dr. Turner.
FOFs are buzzing (and panicking) about last week’s article in The New York Times that examines a body of research from Dr. Martin Mainster and Dr. Patricia Turner, two ophthalmologists from the University of Kansas School of Medicine. Mainster and Turner claim that the gradual yellowing of the lens and narrowing of the pupil that occur with age prevent sunlight from getting through to key cells in the eye. They claim that this disturbs our circadian rhythms–the body’s natural clock–and leaves us at greater risk for a number of ailments, including insomnia, heart disease, cancer and depression. Their evidence is compelling: Based on their research, Mainster and Turner estimate that by age 45, the average adult receives just 50 percent of the light needed to fully stimulate the circadian system. By age 55, it dips to 37 percent and by age 75, to a mere 17 percent. “We believe the effect is huge,” says Dr. Turner.
The two doctors claim there is much research left to do, however they recommend that as we age we should make an effort to expose ourselves to bright sunlight or bright indoor lighting. They are also wary of cataract surgery that involves the implantation of “blue-blocking” lenses, as these may further limit the critical light that reaches the eye. Mainster and Turner have installed skylights and extra fluorescent lights in their own offices to help offset the effects.
So is it time to panic? Should you install windows in the ceiling or move your office to the front lawn? Not so fast says Dr. Russell Fumuso, MD, an ophthalmologist, surgeon and Founding Partner of Ophthalmic Consultants of Long Island (OCLI), one of the largest ophthalmology practices in the country. “The article sounds very dire,” Dr. Fumoso admits. “If you read it, you might think that as you age, you’re inevitably not going to be able to sleep; you’re going to get depressed….you’re going to become some sort of a zombie. In reality, that’s just not true. Everyone in the world gets cataracts as they age–not everyone experiences these other ailments.”
Fumuso goes on to point out that there are other reasons one begins to see sleep disturbances, heart disease and depression in patients in their 50s…namely, menopause. “The body systems are all interconnected, so looking at the eye as the root of all these problems is . . . problematic. It would be nice if it were the answer to everything, but it doesn’t work that way.”
When it comes to the “blue-blocking” lens implants that Mainster and Turner oppose, Dr. Fumuso says, “That’s the Alcon lens. It’s be implanted in over 26 million people in the last 10 years–that’s a pretty good track record. If you’re concerned, talk to your doctor–there are other options.”
So what can we do to preserve eye health and function as long as possible–if not skylight installation? “Stop smoking!” says Dr. Fumuso. “And eat a healthy diet. Your eyes are a lifetime in the making.”